
Table of Contents
Introduction
HIV/AIDS remains an important public sexual health issue that confronts countries all other the world. HIV/AIDS is caused by the human immunodeficiency virus (VIRUS). At the most initial stage of infection, a person is said to only have HIV (Kizito et al., 2008). Based on lifestyle activities and the use of antiretroviral drugs, a person with HIV develops AIDS after certain period of time. AIDS is the stage of the disease where the immune system is not able to fight new infections and diseases, leading to eventual death of the patient (Coleburnders & Ndumbe, 2013). There remains no known or certified drug for either preventing or healing HIV/AIDS. In this essay, the focus of HIV/AIDS as a public sexual health issue is centred on sub-Saharan Africa.
This region of the world remains of particular interest to the academia, researchers, health professionals and the general public due to its prevailing dynamics about the disease. For example it is known that although the whole of Africa make up only 15.2% of world population, the percentage of people aged 15 to 30 living with HIV in Sub-Saharan Africa alone is 69% (Joint United Nations Programme on HIV and AIDS, 2012). What is even worse is that compared to the UK where death from AIDS remains less than 20%, 70% of all deaths associated with AIDS in the world is known to occur in the Sub-Saharan Africa (Joint United Nations Programme on HIV and AIDS, 2012). This means that compared to the UK, Sub-Saharan do not only have high prevalence rate for HIV/AIDS but that patients do not receive good treatment, leading to early onset of AIDS and eventual deaths.
Analysis of HIV/AIDS in relation to public health and health promotion
Adams et al. (2003) explained that public health involves all programmes and activities put in place for the prevention of diseases to achieve prolonging of life and overall promotion of health through the use of shared responsibility, organised efforts, and informed choices made by individuals and society. Based on this definition, one would appreciate that the issue of HIV/AIDS can be perceived from a public health perspective. That is, public health focuses on three major paradigms, all of which have certain contextual application in HIV/AIDS. The first of these is the fact that public health seeks to prevent diseases. Meanwhile, HIV/AIDS is a preventable health condition (Kebaabetswe et al., 2009). By inference, public health workers can direct their role of preventing diseases at HIV/AIDS and expect to succeed with this. In most parts of the world including UK, the issue of HIV/AIDS prevention is viewed from five major outlooks. These are sexual contact preventions, pre-exposure preventions, post-exposure preventions, mother-to-child prevention, and vaccination (Katz et al., 2009). Wilson and Junger (2008) however noted that the commonest modes of preventing HIV/AIDS in Sub-Saharan Africa is through sexual contact prevention, pre-exposure prevention, and mother-to-child prevention. Indeed sexual contact prevention has been done by promoting consistent use of condom, which is known to reduce risk of transmission by 80% (Hall & Snow, 2016). Mother-to-child prevention in Sub-Saharan Africa is at an impressive rate of 92-99%, which is also the global rate. Post-exposure prevention is however low for victims of sexual assault but may be available for medical professional who suffer needle-stick injuries (Kizito et al., 2008).
The second paradigm of public health is the need to achieve prolonged life. Indeed even though HIV/AIDS is generally not curable and vaccinations are only at the trial stages, it remains a fact that with proper lifestyle and medical care, it is possible for people living with the disease to achieve prolonged life (Klimas, Koneru & Fletcher, 2008). By inference, public health workers can succeed with the paradigm of promoting prolonging of life by focusing on HIV/AIDS. As far as HIV/AIDS is concerned, the need achieve prolonged life is achieved through the treatment of disease after a person has been diagnosed. In terms of treatment, four major avenues are used, which are use of antiviral therapy, opportunistic infections, diet, and alternative medicine (Naicker et al., 2009). In Sub-Saharan Africa, even though all these forms of treatments are available, the use of antiviral therapy is the most common. Using antiretroviral drugs is known to push plasma HIV-RNA count to levels below 50 copies and thus guaranteeing delayed onset of AIDS (Shelton, Cassell & Adetunji, 2005). It is also ideal for achieving pre-exposure prevention and once there is no infection, prolonged life can be guaranteed. The final aspect of public health is promotion of health, which is done in HIV/AIDS by having several organised and shared responsibility to promote informed choices made by individuals and groups (Levine & Oomman, 2009). Such health promotion is mainly done through public education in Sub-Saharan Africa. Such public education may either be government sponsored or undertaken by civil society groups. The media is also instrumental in public education on HIV/AIDS (Smith & Morrison, 2006).
The impact of cultural beliefs and practises on sexual health
The issue of culture and HIV/AIDS continues to be extensively discussed and debated in public discourse and the academia. Based on existing literature, it would be said that it is widely agreed that there is a relationship between culture and HIV/AIDS (Lieberman et al., 2009). However, based on the context of culture, the nature of relationship may be different. In Sub-Saharan Africa, two cultural practices that are mostly discussed in relation to HIV/AIDS are male and female circumcision. In the case of female circumcision, the commonest term used is female genital mutilation (FGM). In research by the World Health Organisation (2015), it was found that male circumcision is an effective method of preventing HIV/AIDS. This claim is further supported by other studies that have specifically stated that circumcision in Sub-Saharan Africa can result in reduction in the acquisition of HIV in heterosexual men by rates ranging between 38% and 66% over a period of 24 months (Siegfried et al., 2009). Based on these research findings, it would be said that there are some cultural practices in Sub-Saharan Africa that impacts on HIV/AIDS positively. In a similar line of argument, Kebaabetswe et al. (2003) noted that as much as there are popular cultural practices such as tattooing in Sub-Saharan Africa, the frequency of such practices is not high and this is a good indication of the prevention of HIV/AIDS through infections related to sharp object injuries.

Whereas circumcision in males have been said to help in the prevention of HIV, the practice in females is rather said to increase rate of infection as it increases the extent of exposure to the disease. In one study, Denison et al. (2008) noted that in the practice of FGM, it is common to find that devices and equipment used are not sterilised or treated. The practice of FGM involves the deliberate mutilation or removal of the female genitalia. The practice is very common in Sub-Saharan Africa even though in most countries it is considered illegal (USAID, 2006). Coffee et al. (2015) observed that legal actions taken towards the practice has helped in reducing its frequency and contribution to HIV/AIDS but there were moments in the history of the continent when this was a major issue. For example a study by Brady in 1999 found that there were 2 million girls who were subjected to FGM in Sub-Saharan Africa. What is particularly regrettable is that FGM have been confirmed to be associated with several sexual health problems. Key among is HIV/AIDS (Johnson et al., 2011). In the same study by Brady, it was found that 22 to 44% of all circumcised women admitted to hospitals had pelvic inflammatory disease and other forms of STIs. Meanwhile, these STIs put the women at high risk of contracting HIV.
Another cultural believe that is of prime worry in Sub-Saharan Africa is the fact that there continues to be a good number of people who perceive HIV/AIDS to be a spiritual disease. To such people, those who get HIV/AIDS are cursed in one way or the other (Hallet et al., 2007). Because of such cultural believes, it has always been the case that people living with HIV/AIDS (PLWHA) are either neglected or stigmatised against. Meanwhile, Duffy (2005) lamented about the problem of stigmatisation, blaming it as a major factor leading to poor quality of life and low wellness among PLWHA. In a similar line of argument, Leclerc-Madlala (2008) opined that even in cases were PLWHA are not stigmatised against due to the cultural believe of spiritualism, there is a common sense of reasoning that HIV/AIDS is only a disease for promiscuous people.
Legal, ethical, clinical and political implications of HIV/AIDS from an international perspective
Due to the extent of seriousness attached to the issue of HIV/AIDS at the international level, there are a number of legal, ethical, clinical, and political implications attached to issues concerning it. One such implication is the issue of access to care. At the international level, and as widely accepted in Sub-Saharan Africa, access to care for PLWHA is incorporated as a major legal, clinical and political issue (Boxall & Smith, 2004). From a more legal and political perspective, access to care is incorporated into the larger human rights of PLWHA. That is, as much as other healthy people are seen to have the right to healthcare, so are PLWHA expected to have (Bailey, Plummer & Moses, 2001). The implication of this is that in the dissemination of healthcare, no one would have the power to relegate PLWHA to the background due to their conditions. Marks et al. (2015) opined that access to care for PLWHA also has several clinical implications for patients. That is, due to the promotion of access to care, the overall quality of life of patients is said to have improved tremendously over the past decade in Sub-Saharan Africa. In a study by Anglewicz and Kohler (2009), it was found that as part of discrimination in care, PLWHA did not have the boldness to come forward for treatment. But with the advancement of access to care, this situation has changed tremendously.
The second issue with legal and ethical implication on HIV/AIDS is discrimination and social stigma. At the international level and as practiced in countries across the globe, there are specific laws making it criminal to discriminate against people based on their HIV/AIDS status (Adams et al., 2013). Even though most countries do not have laws specifically mentioning discrimination against PLWHA, they have other legislations and laws that frown on discrimination in general. Auvert et al. (2005) observed that before laws against discrimination started focusing on PLWHA at the international level, it was common to experience social discriminations that extended to such settings as the labour market. For this reason, it often became difficult for such people to get jobs they were duly qualified for based on their HIV status. In a related line of argument, King et al. (2009) underscored the fact that stigmatisation against PLWHA was very common when the promotion for the social protection of such people was low. Through massive international and national campaigns against discrimination, the extent of stigmatisation against PLWHA is reported to have been generally curtailed. In a study by Bailey et al. (2007) most repondents who were HIV negative admitted that they find it ethically inappropriate to discriminate against PLWHA. Such claims underscore the extent to which campaigns aimed at the reduction of discrimination has succeeded.
Another important political implication currently associated with HIV/AIDS is an admission to the contribution of PLWHA to national economy. Burns et al. (2015) emphasised that in early years of HIV/AIDS, it was very common for people contracting HIV to experience the deterioration of their health at very early stages. It was often the case that AIDS set in for people with HIV in as little time as three years. For this reason, it was common to find people losing their lives after only five years of being diagnosed with HIV. This situation had a lot of implications on the contribution that PLWHA made to the national economy. That is, because of the deplorable state of health of the PLWHA, it was often very difficult for them to actively contribute their human capital to the development of national economies through increased productivity at the workplace (Collier et al., 2007). Much of this situation has however changed today. Due to advanced knowledge in the treatment of HIV/AIDS, PLWHA live more healthy lifestyles, much of which is similar to the kind of lifestyle lived by all other healthy individuals. Because of this, such PLWHA are able to go about their regular economic activities, guaranteeing their place of productivity to national development (Corbett et al., 2007). Charalambous et al. (2004) argued that as a result of the increased contribution of PLWHA to national economies, there are now political implications where their place in national development is widely respected and protected.
National and International interventions that address HIV/AIDS
As far as Sub-Saharan Africa and HIV/AIDS among people aged 15 to 30 years is concerned, greater aspect of national interventions were focused on sexual prevention. Consequently, the ABC of HIV/AIDS was largely used as an intervention. The ABC intervention stands for Abstinence, Be Faithful and Condom use (Liddicoat et al., 2016). That is, people were admonished to abstain from all forms of sexual activities as a strategy to protect themselves against HIV/AIDS. The component of abstinence was mostly targeted at young unmarried people (Leclerc-Madlala, 2008). The second component of being faithful targeted married people and the need for them not to keep multiple sexual partners or engage in any extra-marital affairs. This was also seen as a means by which the rate or extent of transmission could be reduced among such married people, whether they were already diagnosed or with HIV or were HIV negative. In the final paradigm of condom use, people who felt they could neither abstain nor be faithful were admonished to use condoms to protect themselves from contracting HIV/AIDS. The basis for the last paradigm on condom use was based on the outcome of research showing that continuous use of condom was effective in reducing the risk of getting infected by over 90% (Corbett et al., 2006).
Today, the ABC intervention is still in use but its frequency of use has been reduced and replaced with what is perceived as a more efficable intervention known as the combination prevention. Combination prevention intervention is an internationally recognised strategy for preventing HIV/AIDS which works through the combination of behavioural, biomedical and structural interventions as explained in detail in the figure below.
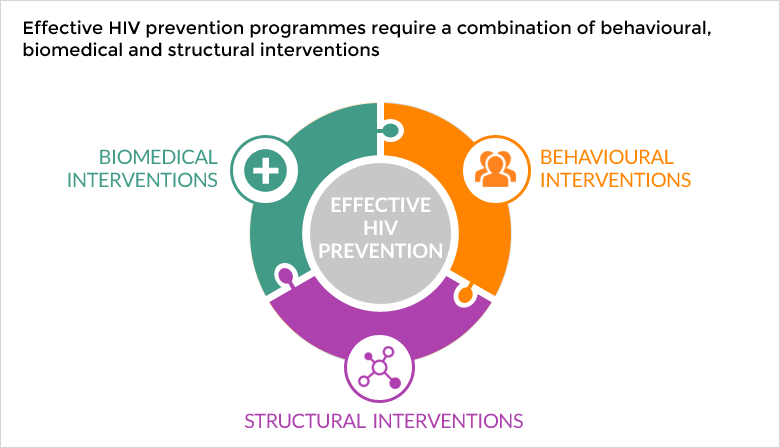
From the figure, it would be noted that the combination prevention combines three different interventions. The first intervention which is biomedical interventions seeks to use biological and medical advancements to prevent HIV. As mentioned earlier, there are both pre-exposure and post-exposure prevention modalities which are based on the use of various medications given to people exposed to HIV either at the earlier stage of infection or later periods (Dinh et al., 2005). On the whole, the biomedical interventions seek to suppress the chances of infecting partners in people who have HIV but with CD4 count of either equal to or less than 550 cells/µL (deWit & Adam, 2008). With those whose CD4 count exceed 550 cells/µL, biomedical interventions ensure there is no further deterioration of the CD4 count. Behavioural interventions on the other hand seek to promote healthy lifestyles that minimises the risk of new infections and re-infections (Gray et al., 2007). Conaty et al. (2015) stressed that with structural interventions, institutions are empowered both at the governmental and non-governmental levels to ensure there is adequate advocacy and education on HIV/AIDS.
Conclusion
From the essay, it has been established that the fight against HIV/AIDS in Sub-Saharan Africa is a process rather than an event. What is implies is that the need to ensure maximum prevention of this health issue, while improving the quality of life of people with the condition is an attainable situation but it is only going to take happen when series of measures are put in place. In the current circumstance, the state of HIV/AIDS prevention and public health in Sub-Saharan Africa is not as effective as what is seen in developed countries such as UK. However, based on the different preventive interventions as well as approach to treatments seen in the paper, it can be perceived that it will not be long for the region to catch up with other parts of the world. But in order to speed up the process, it will be important that such cultural practices such as FGM will be repelled with strong backing in law. It is also important to see HIV/AIDS strictly as a public health issue rather than a spiritual one. This way, the need to use more orthodox means in addressing the condition can be enhanced.
- Adams AL et al. (2013) ―HIV infection risk, behaviors, and attitudes about testing: are perceptions changing?. Sexually Transmitted Disease 30(10): 764 -768.
- Anglewicz P & Kohler H.P (2009) ―Overestimating HIV infection: The construction and accuracy of subjective probabilities of HIV infection in rural Malawi. Demographic Research 20(6): 65-96.
- Auvert B et al. (2005) ―Randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk: The ANRS 1265 Trial.: PLoS Medicine 2(11): 1,112-1,22.
- Bailey, RC et al. (2007) ―Male circumcision for HIV prevention in young men in Kisumu, Kenya: A randomized controlled trial.. Lancet 369(9562): 643 – 656.
- Bailey, RC, Plummer FA & Moses S (2001) ―Male circumcision and HIV prevention: current knowledge and future research directions.. The Lancet Infectious Disease 1: 223 – 230.
- Boxall EH. & Smith N. (2004). ―Antenatal screening for HIV; are those who refuse testing at higher risk than those who accept testing?. Journal of Public Health 26(3): 285-287.
- Brady, M. (1999). Female genital mutilation: Complications and risk of HIV transmission. ADIS Patient Care and STDs. Vol. 13 No. 12, pp. 709-716
- Burns, F. et al. (2015). “Factors that may increase HIV testing uptake in those who decline to test (vol 80, pg 249, 2004).” Sexually Transmitted Infections 81(1): 94.
- Charalambous S, Grant AD, Day JH, Rothwell E, Chaisson RE, Hayes RJ, Churchyard GJ. (2004) ―Feasibility and acceptability of a specialist clinical service for HIV-infected mineworkers in South Africa. AIDS Care 16(1):47-56.
- Coates T, et al. (2000). Voluntary HIV-1 Counseling and Testing Efficacy Study Group. Efficacy of voluntary HIV-1 counseling and testing in individuals and couples in Kenya, Tanzania, and Trinidad: a randomized trial. The Lancet 356: 103-112.
- Coffee, P et al. (2015) ―Patterns of movement and risk of HIV infection in rural Zimbabwe. Journal of Infectious Diseases 191 (Supplement 1): S159 -167.
- Coleburnders R & Ndumbe P (2013) ―Priorities for HIV testing in developing countries?. The Lancet 342:610-602.
- Collier AC, Van der Borght SF, Rinke de Wit T, Richards SC, Feeley FG. (2007) ―A successful workplace program for voluntary counseling and testing and treatment of HIV/AIDS at Heineken, Rwanda. International Journal of Occupational and Environmental Health 13(1):99-106
- Conaty, S. J. et al. (2015). “Women who decline antenatal screening for HIV infection in the era of universal testing: results of an audit of uptake in three London hospitals.” Journal of Public Health 27(1): 114-117.
- Corbett EL et al. (2006) ―Uptake of workplace HIV counselling and testing: a cluster- randomised trial in Zimbabwe. PLoS Med 3(7) :e238.
- Corbett EL, Makamure B, Cheung YB, Dauya E, Matambo R, Bandason T, Munyati SS, Mason PR, Butterworth AE, Hayes RJ. (2007) ―HIV incidence during a cluster-randomized trial of two strategies providing voluntary counselling and testing at the workplace, Zimbabwe. AIDS 21(4):483-9.
- Denison JA, O’Reilly KR, Schmid GP, Kennedy CE, and MD Sweat (2008) ―HIV voluntary counseling and testing and behavioral risk reduction in developing countries: a meta-analysis, 1990—2005. AIDS Behavior 12(3):363-73.
- deWit JB & Adam PC (2008) ―To test or not to test: psychosocial barriers to HIV testing in high-income countries. HIV Medicine 9 Supplement 2:20-22.
- Dinh T. H. R. et al. (2005). “Factors associated with declining HIV testing and failure to return for results among pregnant women in Vietnam.” Aids 19(11): 1234-1236.
- Duffy, L (2005). Cultural and context of HIV prevention in rural Zimbabwe: the influence of gender inequality. Journal of Transcultural nursing 16: 23-31.
- Gray RH et al. (2007) ―Male circumcision for HIV prevention in men in Rakai, Uganda: A randomized trial. Lancet 369(9562): 657-666.
- Hall GJ & Snow RC (2016)―Patterns in HIV testing and receiving test results among sub-Saharan African women and men: An examination of the Demographic and Health Survey Data from 2003-2007 Forthcoming
- Hallet TB et al. (2007) ―Age at first sex and HIV infection in rural Zimbabwe.. Studies in Family Planning 38(1):1-10.
- Johnson AM et al., (2011) ―Sexual risk behavior in Britain: partnerships, practices, and HIV risk behaviors. Lancet
- Joint United Nations Programme on HIV and AIDS (2012). Global fact sheet. [Online] Available at http://files.unaids.org/en/media/unaids/contentassets/documents/epidemiology/2012/gr2012/20121120_FactSheet_Global_en.pdf [November 17, 2016]
- Katz DA, Kiarie JN, John-Stewart GC, Richardson BA, John FN and C Farquhar (2009) ―Male perspectives on incorporating men into antenatal HIV counseling and testing. PLoS One 4(11):e7602.
- Kebaabetswe P et al. (2009) ―Perceptions of couple HIV counseling and testing in Botswana: A stakeholder analysis. Patient Education and Counseling 79(1):120-123.
- Kebaabetswe P, Lockman S, Mogwe S, Mandevu R, Thior I, Essex M and RL Shapiro (2003) ―Male circumcision: an acceptable strategy for HIV prevention in Botswana. Sexually Transmitted Infections. 79: 214-219.
- King R et al. (2009) ―The virus stops with me: HIV-infected Ugandans‘ motivations in preventing HIV transmission. Social Science and Medicine 68: 749-757.
- Kizito D et al. (2008) ―Uptake of HIV and syphilis testing of pregnant women and their male partners in a programme for prevention of mother-to-child HIV transmission in Uganda. Tropical Medicine and International Health 13(5):680-682.
- Klimas N, Koneru AO & Fletcher MA (2008). Overview of HIV. Psychosomatic Medicine 70: 523-530.
- Leclerc-Madlala S (2008) ―Age-disparate and intergenerational sex in southern Africa: the dynamics of hyper-vulnerability. AIDS 22 (Supplement 4): S17-S25.
- Levine R & Oomman N (2009) ―Global HIV/AIDS funding and health systems: Searching for the win-win JAIDS 52(Supplement 1): S3 – S5.
- Liddicoat R V et al. (2016) ―Refusing HIV testing: High-risk behavior or risk- reduction strategy?. AIDS 14: 547 – 552.
- Lieberman S., Gottret P., Ye E., de Beyer J., Oelrich R., and D Zewdie (2009) ―International health funding and the response to AIDS. JAIDS 52(Supplement 1): S38 – S44.
- Marks G, Crepaz N, Senterfitt JW, & Janssen RS (2015) ―Meta-analysis of high-risk sexual behavior in persons aware and unaware they are infected with HIV in the United States: implications for HIV prevention programs. Journal of Acquired Immunodeficiency Virus 39(4) :446-53.
- Naicker S., Plange-Rhule J., Tutt RC., and JB Eastwood (2009) ― Shortages of healthcare workers in developing countries – Africa. Ethnicity and Disease 19(Supplement 1):S1-60–S1-64.
- Shelton JD, Cassell MM, & Adetunji J (2005) ―Is poverty or wealth at the root of HIV?. The Lancet 366(9491):1057-8.
- Siegfried, N., Muller, M., Deeks, J.J. & Volmink, J. (2009). “Male circumcision for prevention of heterosexual acquisition of HIV in men”. Cochrane database of systematic reviews (Online) (2): CD003362.
- Smith RA & Morrison D (2006) ―The impact of stigma, experience, and group reference on HIV risk assessments and HIV testing intentions in Namibia.. Social Science and Medicine 63(10): 2649 -2660.
- USAID (2006) AIDS epidemic update. Geneva
- Wilson JMG & Junger G (2008) Principles and Practices of Screening for Disease Public Health Paper -34 World Health Organization Geneva
- World Health Organisation (2015). HIV/AIDS fact sheet. [Online]