
Table of Contents
Introduction
The connection that exists between the ovarian cysts and infertility that takes place amongst women is a debatable subject for the primary fact that it is hard to identify the actual impact they have on later infertility. An ovarian cyst refers to a sac filled with fluids in the ovary of a woman. The cysts vary in size and most cases they could be 1 to 4 centimeters (Byron Redwine, 2015). The liquid inside the cyst could also differ in the manner that it could be watery or paste-like. In a few cases, the ovarian cysts could grow up to 5 centimeters or even more. The population of women that could probably have ovarian cysts at some point in their lives includes women who have already gone through puberty and are at the childbearing stage that is between the ages 18-45. The objective of this paper is to explore the subject of ovarian cysts thoroughly and identify the relationship that it has with infertility in women.
Ovarian cysts could occur between the mentioned productive ages, but the diagnosis is most common for women who are in their middle ages, the twenties, and the thirties. However, the diagnosis could be made as early as when a young woman is just at the onset of her puberty that is at around 11 years (Byron Redwine, 2015). Many ovarian cysts never make a woman uncomfortable or instead prove to be harmless. Every woman consists of two ovaries one at each side of her uterus. The primary purpose of these ovaries is to aid the woman to produce eggs for fertilization during reproduction. Therefore, the ovaries function to produce progesterone and estrogen, which are the primary hormones that lead to the menstrual cycle in a woman.
Every month a woman has to ovulate meaning that one of the ovaries on each side of the uterus has to produce an egg for fertilization. If these ovaries do not provide the eggs for fertilization, then there is a high chance of an ovulation problem that might result in the formation of cysts. Difficulties regarding ovulation including cysts are responsible for 25 percent of all the female infertility problems. Most ovarian cysts are prevalent in women who are obese especially the complex ones such as the Polycystic Ovarian Syndrome which has high chances of leading to infertility.
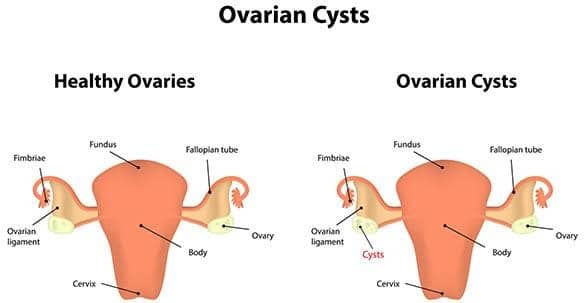
Fig 1.0 showing Ovarian Cysts

Pathology of Ovarian Cysts
Studies done by Mavrelos, & Saridogan (2015) Problems with the ovulation cycle are the main reasons as to why cysts are very common in the ovaries. In normal circumstances when a woman is healthy with no ovulation problem, the follicle still consists of fluid. The follicle should be able to rupture when the ovary releases the egg, and if it does not, it gets bigger since the fluid is not dischargeable. Consequently, the swelling follicle becomes cysts known as functional cysts because it has occurred because of the ovarian function. A corpus luteum is another cyst that results from the role of the ovaries. This type of a cyst occurs when blood or any fluid fills the corpus lutetium. Suppose a bleeding occurs in any of the functional cysts then it is a hemorrhagic cyst.
A majority of the women who suffer from the ovulation problems entailing endometriosis also have the ovarian cysts. These type of cysts are commonly referred to as chocolate cysts because of the old dark blood contained in them. Women who have PCOD (Polycystic Ovarian Disease) are most likely to have cysts too. Consequently, in a few circumstances, the dermoid cysts may develop. This type of a cyst consists of a variety of tissues including skin, or hair (Alebić, Stojanović, Baldani, & Duvnjak, 2017). Dermoid cyst stems from the cells that create the eggs entailed in the ovaries.
Dermoid cysts are more prevalent in women who are younger as compared to those who are a bit older. A cystadenoma, on the other hand, is a cyst that occurs from the cells covering the exterior part of the ovary. Different types of a cystadenoma exist including those filled with serous cystadenoma (watery liquid) and those filled with mucinous cystadenoma (thick mucus substance) (Alebić, Stojanović, Baldani, & Duvnjak, 2017). Other than the functional cause of the ovarian cysts, doctors also attribute this condition to genetics where women who have sisters and mothers who have the disease are more likely to acquire it.
Epidemiology of the Ovarian Cysts
Different scholars stipulate that the prevalence of ovarian cysts range between 8 to 18 percent entailing both the premenopausal and postmenopausal women. In the United States of America, about 5 to 10 percent of women in their reproductive years (Premenopausal) seek surgical exploration to remove the cysts present in their bodies (Byron Redwine, 2015). Scientists in their assessments have discovered that approximately ten percent of the ovarian cysts in women are malignant. Pre-surgical examination of the ovarian cysts is crucial to avoid any surgical intervention that might not be necessary. The pre-surgical evaluation also assists in the detection of possible malignancy.
In many women, the ovarian cysts present in their ovaries are not precancerous lesions and are highly unlikely to increase the chances of developing ovarian cancer in the future, and their removal does not decrease the mortality rate of ovarian cancer in the future also (Baldani, Skrgatic, & Ougouag, 2015). In most cases, the ovarian cysts do not pose any danger to the health of the women because most of them are not cancerous as mentioned before. Many of these ovarian cysts occur because of the process of menstruation, and for this reason, they are most likely heightened by hormonal problems, pregnancy, endometriosis, previous ovarian cyst and severe pelvic infection.
Hormonal problems, which entail taking clomiphene, which is a fertility drug, may result in the cysts. Occasionally, the cyst may form when a woman ovulates and therefore stay on the ovary throughout a woman’s pregnancy. On the other hand, Endometriosis refers to a condition the results in the growth of the endometrial cells out of the uterus and afterward attach to the ovary causing the formation of cysts (Alebić, Stojanović, Baldani, & Duvnjak, 2017). Severe pelvic infections lead to the existence of ovaries and in most cases, when one had a cyst before, and then they are most likely to develop more cysts.
Symptoms of Ovarian Cysts
In many cases, the ovarian cysts do not cause any symptoms. When the ovarian cysts hardly cause any symptoms, it is highly recommended to ignore them. In other times, some of the ovarian cysts may result in an irregular menstrual bleeding, and when they are hormonally active, and then there is a high chance that they can cause pelvic pain. However, ovarian cysts can only result in pain if they are too big to the extent that they exert much pressure on the surrounding structures and the ovary itself (Barthelmess, & Naz, 2014). In such a case a dull ache will occur. In addition, in cases where the cyst bleeds there does the patient experience a sharp and intense pain?
In sporadic cases, twisting might occur in an ovarian cyst making it cut off its blood supply in a process known as a torsion. This process causes vomiting, fever, and abdominal pain and highly requires medical attention. Cases where the cysts burst are also frequent and as a result cause pain in the lower abdomen. Pain resulting from the bursting of the cysts is severe and sudden. However, the sharpness of the pain that a woman experiences from the ovarian cysts depends on whether the cyst is bleeding or infected.

In general terms, the most common symptoms that women might experience when they have ovarian cysts include, discomfort experienced in the lower abdomen, severe pain that occurs because of a cyst rupture and pain during intercourse precisely when there is a deep penetration. There are alterations in the bowel movements including constipation; menstrual irregularities are also common, bloating, and abdominal fullness. The patient may also experience pelvic pressure, which may result in urinary frequency, heartburn, indigestion, and endometriomas (Barthelmess, & Naz, 2014). Endometriomas occurs because of endometriosis which results in heavy, painful periods. The ovarian cysts may also result in hypertension, hyperpyrexia, and cervical motion tenderness.
Implications of Ovarian Cysts on Fertility
Studies done by different scholars show that ovarian cysts do not prevent a woman from getting pregnant, but they can make the process of conceiving a little more difficult. Infertility is a severe medical condition whereby it affects approximately 7.3 million women in America (Kim, Lee, Lee, Jo, Moon, Shin, Jeon, 2014). Ovarian cysts can interfere with the capability of a woman to ovulate, which is the primary process as explained earlier needed for a woman to conceive.
The irregularities that take place when it comes to ovulation are the main reasons for a quarter of the cases involving infertility in women. Some ovarian cysts cause infertility while others do not cause infertility. For this reason, the implication of the ovarian cysts on infertility highly depends on the type of the ovarian cyst that a woman has. The types of ovarian cysts that are highly likely to cause infertility in women include endometriomas and ovarian cysts that occur because of Polycystic Ovary Syndrome. These two types of cysts are highly associated with irregular ovulation.
Irregular ovulation decreases the chances of an egg fertilization and therefore increases the chances of infertility. Functional cysts, cystadenomas, and dermoid cysts are highly unlikely to cause infertility in women unless they swell too much and become too large (Benschop, Farquhar, van der Poel, & Heineman, 2010). In most cases, the presence of these cysts shows that the ovaries are performing their function and that the necessary processes needed for fertility are taking place.
Diagnosis of Ovarian Cysts
It is not easy to tell if a woman has an ovarian cyst since as mentioned before, it is highly unlikely for these cysts to present symptoms in a patient. For this reason, ultrasound scanning is a critical diagnosis method that can significantly help identify if a woman has ovarian cysts. The resolution and the quality of the ultrasound scanners make it possible for the medical practitioners to diagnose the smallest cysts that might be occurring in a woman’s body. In cases where the cysts are large, the need for an abdominal scan is core so that the size can be identified (Pavone, Hirshfeld-Cytron, Tingen, Thomas, Lowe, Woodruff, 2014). The part of the ovary where the cysts exist and the size are significantly examined using the vaginal ultrasound scan.
The primary reason as to why the ultrasound scan is preferred for the diagnosis of the ovarian cysts is that it is a safe and painless procedure. The ultrasound scanning entails the utilization of sound waves to form images of the organs inside the body of the patient. The doctor can put the probe of the scanner on the abdomen of the woman to get an image of the ovaries of the patient. The medical practitioner can also put a small probe inside the vagina to get a good view of the ovaries. Other than performing the ultrasound scanning, the doctor might also take the urine and blood samples of the patient for examination, or in other cases, an MRI or a CT scan might be necessary.
Diagnosis of ovarian cysts using the ultrasound scan allows the doctors to get a clear image, which they can use to examine the contents of the type of cysts the patient has. Depending on the appearance of the ultrasound, cysts exist in three classes into including cystic, solid, and complex. A cystic cyst consists of a wall, and its contents entail only the fluid. The solid cysts consist of many echoes in it because it only consists of solid tissue. The complex cyst, on the other hand, consists of a combination of both the solid tissue and the fluids. Complex cysts should much attention since they are the ones that could lead to infertility. For this reason, additional tests including the blood tests will help to examine the level of CA-125 (Pavone, Hirshfeld-Cytron, Tingen, Thomas, Lowe, Woodruff, 2014). CA-125 is a blood test. The levels of CA-125 are higher amongst the women who already have ovarian cysts.
Treatment of Ovarian Cysts
In all the cases involving ovarian cysts, approximately 85 percent of them are solvable through the administration of medicine or surgery. However, many doctors may use the wait and see approach whereby the medical practitioner advice the patient to wait for a few months without treatment to see if the cyst will disappear on its own. This treatment approach is most significant for pre-menopausal women who have small functional cysts. After the wait, there is the need of another ultrasound scan to identify if the small cysts occurring because of the functions of the ovary went away (Kim, Lee, Lee, Jo, Moon, Shin, Jeon, 2014). The use of the birth control pills is another method that can help in the treatment of the ovarian cysts. The birth control method works by making the functional cysts smaller and minimizing the chances of the emergence of the new cysts.
Vaginal ultrasound-guided aspiration can help to treat a simple cyst. The process allows the medical practitioner to empty the fluid contents of the cysts, which ends up treating the condition. Laparoscopic surgery is a recommended treatment if the ovarian cysts swell too much and become more than 5cm in size, consists of solid material, results in severe symptoms and last longer than about three menstrual cycles (Sam, Scoccia, Yalamanchi, & Mazzone, 2015). If the cyst is benign (non-cancerous), then the doctor will only remove it. However, if it is cancerous, then the doctors might need to remove the entire ovary. The removal of a cyst using the laparoscopic surgery requires a skilled surgeon regardless of whether the cyst is small or large. The reason why the operation involves expertise is that irrespective of the size, the cysts could be decompressed laparoscopically and as a result cause it to collapse. When the cysts collapse, its walls can be removed using keyhole incision, which means that the patient does not have to go for major surgery.
Laparoscopic surgery is the most preferred treatment for the women who are infertile because the normal ovarian tissue is preserved in the process, which in turn protects the regular function of the ovaries. In rare cases, the doctors use open surgery if the cyst is complex or even solid. Many women who have uncomplicated ovarian cysts realize that the ultrasonographic assessment does not necessarily need treatment. Small cysts that occur because of the functions of the ovaries where the CA-125 count is normal may only require regular monitoring and no further treatment using the ultrasonographic examinations (Kim, Lee, Lee, Jo, Moon, Shin, Jeon, 2014). Pharmacological therapy is also essential for the treatment of ovarian cysts whereby the patient receives oral contraceptive pills to prevent the formation of more cysts and reduce the chances that the cysts may occur again.
Conclusion
In conclusion, there is a connection between the ovarian cysts and infertility in women in their reproductive ages. The fact is that not all the types of the ovarian cysts cause infertility in women. The ovarian cysts that occur because of the function of the ovaries are highly unlikely to cause infertility in a woman. The complex ovarian cysts such as the endometriosis are the main cysts that have the high chances of making a woman infertile. The main reason as to why these cysts cause infertility is that they interfere with the normal functioning of the ovaries creating irregular ovulation (Mavrelos, & Saridogan, 2015). Irregular ovulation consequently results in slim chances of the fertilization of the eggs released from the ovary.
We can do it today.
A proper diagnosis is required to identify the type of a cyst that a woman has. Ultrasound scanners determine the type and size of the cysts present on the ovary of the woman by providing images showing the structures in the woman body. After the diagnosis, the medical practitioner can then decide the most significant method to use to treat the patient. In cases where the cysts are not severe, then the doctor may choose to use the watch and see approach. However, if the cysts identified after the diagnosis are solid or complex, then it means that the need for a surgery mostly the laparoscopic surgery is core.
It is important to realize that most of the ovarian cysts are benign or rather non-cancerous especially for women who are at their pre-menopausal age. However, it is important for a woman to seek treatment as soon as possible because at post-menopausal phase the ovarian cysts have high chances of becoming cancerous. The need for early treatment regardless of whether the ovarian cyst is small or big is core. Early treatment can help reduce the symptoms of the ovarian cysts and reduces the chances of the patient developing other chronic illnesses such as diabetes and hypertension. In addition, it is essential to maintain a proper diet and do exercises, as obesity is one of the major contributors to the ovarian cysts.
- Alebić, M., Stojanović, N., Baldani, D., & Duvnjak, L. (2017). Metabolic implications of menstrual cycle length in non-hyperandrogenic women with polycystic ovarian morphology. International Journal Of Basic And Clinical Endocrinology, 55(3), 798-807. http://dx.doi.org/10.1007/s12020-016-1062-y
- Ashrafi, M., Fakheri, T., Kiani, K., Sadeghi, M., & Akhoond, M. R. (2014). Impact of The Endometrioma on Ovarian Response and Pregnancy Rate in In Vitro Fertilization Cycles. International Journal of Fertility & Sterility, 8(1), 29–34.
- Ashrafi, M., Sadatmahalleh, S., Akhoond, M., & Talebi, M. (2016). Evaluation of Risk Factors Associated with Endometriosis in Infertile Women. International Journal Of Fertility And Sterility, 11(21).
- Baldani, D. P., Skrgatic, L., & Ougouag, R. (2015). Polycystic Ovary Syndrome: Important Underrecognised Cardiometabolic Risk Factor in Reproductive-Age Women. International Journal of Endocrinology, 2015, 786362. http://doi.org/10.1155/2015/786362
- Balen, A., Morley, L., Misso, M., Franks, S., Legro, R., & Wijeyaratne, C. et al. (2016). The management of anovulatory infertility in women with polycystic ovary syndrome: an analysis of the evidence to support the development of global WHO guidance. Human Reproduction Update, 22(6), 687-708. http://dx.doi.org/https://doi.org/10.1093/humupd/dmw025
- Barthelmess, E. K., & Naz, R. K. (2014). Polycystic ovary syndrome: current status and future perspective. Frontiers in Bioscience (Elite Edition), 6, 104–119.
- Bates, G. W., & Legro, R. S. (2013). Longterm management of Polycystic Ovarian Syndrome (PCOS). Molecular and Cellular Endocrinology, 373(0), 91–97. http://doi.org/10.1016/j.mce.2012.10.029
- Benschop, L., Farquhar, ,., van der Poel, N., & Heineman, M. (2010). Interventions for women with endometrioma prior to assisted reproductive technology. Cochrane Database Of Systematic Reviews, (11). http://dx.doi.org/10.1002/14651858.CD008571.pub2
- Brauner, R., Bashamboo, A., Rouget, S., Goulet, M., Philibert, P., Sarda-Thibault, H., … McElreavey, K. (2010). Clinical, Biological and Genetic Analysis of Prepubertal Isolated Ovarian Cyst in 11 Girls. PLoS ONE, 5(6), e11282. http://doi.org/10.1371/journal.pone.0011282
- Bremer, A. A. (2010). Polycystic Ovary Syndrome in the Pediatric Population. Metabolic Syndrome and Related Disorders, 8(5), 375–394. http://doi.org/10.1089/met.2010.0039
- Byron Redwine, D. (2015). Ovarian endometriosis: a marker for more extensive pelvic and intestinal disease. Fertility And Sterility, 72(2), 310-315. http://dx.doi.org/http://dx.doi.org/10.1016/S0015-0282(99)00211-3
- Choi, P.-W., Yang, J., Ng, S.-K., Feltmate, C., Muto, M. G., Hasselblatt, K., … Ng, S.-W. (2016). Loss of E-cadherin disrupts ovarian epithelial inclusion cyst formation and collective cell movement in ovarian cancer cells. Oncotarget, 7(4), 4110–4121. http://doi.org/10.18632/oncotarget.6588
- Dumitrescu, R., Mehedintu, C., Briceag, I., Purcarea, V., & Hudita, D. (2015). The Polycystic Ovary Syndrome: An update on metabolic and hormonal mechanisms . Journal of Medicine and Life, 8(2), 142–145.
- Dunaif, A. (2016). Perspectives in Polycystic Ovary Syndrome: From Hair to Eternity. The Journal of Clinical Endocrinology and Metabolism, 101(3), 759–768. http://doi.org/10.1210/jc.2015-3780
- El Hayek, S., Bitar, L., Hamdar, L. H., Mirza, F. G., & Daoud, G. (2016). Poly Cystic Ovarian Syndrome: An Updated Overview. Frontiers in Physiology, 7, 124. http://doi.org/10.3389/fphys.2016.00124
- Emeksiz, H. C., Derinöz, O., Akkoyun, E. B., Güçlü Pınarlı, F., & Bideci, A. (2017). Age-Specific Frequencies and Characteristics of Ovarian Cysts in Children and Adolescents. Journal of Clinical Research in Pediatric Endocrinology, 9(1), 58–62. http://doi.org/10.4274/jcrpe.3781
- Ingrid Dravecká, I. (2016). CLINICAL EFFECTS OF SYNDRODE OF POLYCYSTIC OVERS, 65(2), 392-397.
- Iwase, A., Nakamura, T., Nakahara, T., Goto, M., & Kikkawa, F. (2014). Assessment of ovarian reserve using anti-Müllerian hormone levels in benign gynecologic conditions and surgical interventions: a systematic narrative review. Reproductive Biology and Endocrinology : RB&E, 12, 125. http://doi.org/10.1186/1477-7827-12-125
- Kalra, G., Campbell, S., & Nargund, G. (2016). Ovarian reserve may be compromised after adnexal surgery: Are we sufficiently fertility- focused in our surgical training? Facts, Views & Vision in ObGyn, 8(2), 104–108.
- Kim, J. H., Lee, S. M., Lee, J.-H., Jo, Y. R., Moon, M. H., Shin, J., … Jeon, H. W. (2014). Successful Conservative Management of Ruptured Ovarian Cysts with Hemoperitoneum in Healthy Women. PLoS ONE, 9(3), e91171. http://doi.org/10.1371/journal.pone.0091171
- King, J. (2017). Polycystic Ovary Syndrome. Journal Of Midwifery Womens Health, 51(6), 415-422. http://dx.doi.org/https://doi.org/10.1016/j.jmwh.2006.01.008
- KOSOVA, G., & URBANEK, M. (2013). GENETICS OF THE POLYCYSTIC OVARY SYNDROME. Molecular and Cellular Endocrinology, 373(0), 29–38. http://doi.org/10.1016/j.mce.2012.10.009
- Legendre, G., Catala, L., Lacoeuille, C., Boussion,, F., Sentilhes,, L., & Descamps,, P. (2014). Relationship between ovarian cysts and infertility: what surgery and when. Fertility And Sterility, 101(3), 608-614. http://dx.doi.org/http://dx.doi.org/10.1016/j.fertnstert.2014.01.021 show
- Leibson,, C., Good,, A., Hass, S., Ransom, J., Yawn, B., O’Fallon, M., & Melton, J. (2004). Incidence and characterization of diagnosed endometriosis in a geographically defined population. FERTILITY AND STERILITY, 88(2), 314-321.
- Lenart-Lipińska, M., Matyjaszek-Matuszek, B., Woźniakowska, E., Solski, J., Tarach, J. S., & Paszkowski, T. (2014). Polycystic ovary syndrome: clinical implication in perimenopause. Przegla̜d Menopauzalny = Menopause Review, 13(6), 348–351. http://doi.org/10.5114/pm.2014.47988
- Mavrelos, D., & Saridogan, E. (2015). Treatment of Endometriosis in Women Desiring Fertility. Journal of Obstetrics and Gynaecology of India, 65(1), 11–16. http://doi.org/10.1007/s13224-014-0652-y
- McCartney, C. R., & Marshall, J. C. (2016). Polycystic Ovary Syndrome. The New England Journal of Medicine, 375(1), 54–64. http://doi.org/10.1056/NEJMcp1514916
- Nieweglowska, D., Hajdyla-Banas, I., Pitynski, K., Banas, T., Grabowska, O., Juszczyk, G., … Jach, R. (2015). Age-related trends in anti-Mullerian hormone serum level in women with unilateral and bilateral ovarian endometriomas prior to surgery. Reproductive Biology and Endocrinology : RB&E, 13, 128. http://doi.org/10.1186/s12958-015-0125-x
- Palomba, S., Santagni, S., Falbo, A., & La Sala, G. B. (2015). Complications and challenges associated with polycystic ovary syndrome: current perspectives. International Journal of Women’s Health, 7, 745–763. http://doi.org/10.2147/IJWH.S70314
- Pavone, M. E., Hirshfeld-Cytron, J., Tingen, C., Thomas, C., Thomas, J., Lowe, M. P., … Woodruff, T. K. (2014). Human Ovarian Tissue Cortex Surrounding Benign and Malignant Lesions. Reproductive Sciences, 21(5), 582–589. http://doi.org/10.1177/1933719113506498
- Piltonen, T. T., Chen, J. C., Khatun, M., Kangasniemi, M., Liakka, A., Spitzer, T., … Giudice, L. C. (2015). Endometrial stromal fibroblasts from women with polycystic ovary syndrome have impaired progesterone-mediated decidualization, aberrant cytokine profiles and promote enhanced immune cell migration in vitro. Human Reproduction (Oxford, England), 30(5), 1203–1215. http://doi.org/10.1093/humrep/dev055
- Randeva, H. S., Tan, B. K., Weickert, M. O., Lois, K., Nestler, J. E., Sattar, N., & Lehnert, H. (2012). Cardiometabolic Aspects of the Polycystic Ovary Syndrome. Endocrine Reviews, 33(5), 812–841. http://doi.org/10.1210/er.2012-1003
- Sam, S., Scoccia, B., Yalamanchi, S., & Mazzone, T. (2015). Metabolic dysfunction in obese Hispanic women with polycystic ovary syndrome. Human Reproduction (Oxford, England), 30(6), 1358–1364. http://doi.org/10.1093/humrep/dev073
- Santoro, N., Eisenberg, E., Trussell, J. C., Craig, L. B., Gracia, C., Huang, H., … Zhang, H. (2016). Fertility-related quality of life from two RCT cohorts with infertility: unexplained infertility and polycystic ovary syndrome. Human Reproduction (Oxford, England), 31(10), 2268–2279. http://doi.org/10.1093/humrep/dew175
- Şimşek, M., Kuloğlu, T., Pala, Ş., Boztosun, A., Can, B., & Atilgan, R. (2015). The effect of ethanol sclerotherapy of 5 minutes duration on cyst diameter and rat ovarian tissue in simple ovarian cysts. Drug Design, Development and Therapy, 9, 1341–1347. http://doi.org/10.2147/DDDT.S76835
- Tafazoli, M., Fazeli, E., Dadgar, S., & Nematy, M. (2016). The Association of the Dietary Fat and Functional Ovarian Cysts in Women of Reproductive Age Referring to Three Hospitals in Mashhad, Iran, 2014. International Journal of Community Based Nursing and Midwifery, 4(2), 148–156.
- Teede, H., Deeks, A., & Moran, L. (2010). Polycystic ovary syndrome: a complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. BMC Medicine, 8, 41. http://doi.org/10.1186/1741-7015-8-41
- Tehrani, F., Mansournia, M., & Solaymani-Dodaran, M. (2017). Age-specific serum anti-Müllerian hormone levels: estimates from a large population-based sample. The Journal Of International Menopause Society, 17(5), 591-597.
- van Helden, J., & Weiskirchen, R. (2017). Performance of the two new fully automated anti-Müllerian hormone immunoassays compared with the clinical standard assay. Human Reproduction, 30(8), 1918-2006. http://dx.doi.org/10.1093/humrep/dev127
- Welt, C. K., & Carmina, E. (2013). Lifecycle of Polycystic Ovary Syndrome (PCOS): From In Utero to Menopause. The Journal of Clinical Endocrinology and Metabolism, 98(12), 4629–4638. http://doi.org/10.1210/jc.2013-2375
- Winkelman, W. D., Katz, P. P., Smith, J. F., & Rowen, T. S. (2016). The Sexual Impact of Infertility. Among Women Seeking Fertility Care. Sexual Medicine, 4(3), e190–e197. http://doi.org/10.1016/j.esxm.2016.04.001
- Yuqing, Y., Pei, H., Chang, Y., Chen, M., Wang, H., Xie, H., & Yao, S. (2014). The impact of endometrioma and laparoscopic cystectomy on ovarian reserve and the exploration of related factors assessed by serum anti-Mullerian hormone: a prospective cohort study. Journal Of Ovarian Research, 7(108). http://dx.doi.org/https://doi.org/10.1186/s13048-014-0108-0
- Nasiri Amiri, F., Ramezani Tehrani, F., Simbar, M., Mohammadpour Thamtan, R. A., & Shiva, N. (2014). Female Gender Scheme is Disturbed by Polycystic Ovary Syndrome: A Qualitative Study From Iran. Iranian Red Crescent Medical Journal, 16(2), e12423. http://doi.org/10.5812/ircmj.12423