
Table of Contents
Introduction
The surgical intervention considered to be the most important intervention in the treatment plan to preserves patient’s life (Price et al. 2004). Advance scheduling for elective cases in the operating room (OR) is an essential move to make sure patients and OR are well prepared for the surgery (Spry 2009). However, revocations of the elective case are collective incidences globally (Jonnalagadda et al. 2005). Therefore, this negatively affects the hospital and the patients (Ezike et al. 2011). However, Mutwali et al. (2016) notice that, 70.25% of the causes of cancellation were preventable by surgical planning, better administrative and better communications with patients and relatives.
The surgery cancellation on the same day of the surgery may cause several issues in a different level results in additional expenses of the operational and financial aspects, especially regarding direct costs (human resources, material, and medication), lower staff satisfaction (Jonnalagadda et al. 2005). In addition, cancellations can be the primary cause of inconvenience to patients and their relatives, as it will delay treatment, create significant dissatisfaction, significant emotional distress, physiological effects, repeated fasting and extra expenses (Schuster et al. 2011).
The Association of Anaesthetists of Great Britain and Ireland (AAGBI 2003) notice that, the cancellation usually resulting from several issues such as; the surgical problem, delayed starts, shortages of staff, unanticipated anesthetic, turnover, administrative reasons, availability of instruments and over-running lists (ORLs). The ORLs are considered being the main factor that causes cancellations on the surgery-day (Pandit and Carey 2006). It has been reported in different hospitals, which between 10% to 40% of elective cases were canceled before surgery takes place (Kumar and Gandhi 2012).
Typically, in the author hospital, the main factor that leads to the same-day cancellation of elective cases is the ORLs. Several issues can be explored regarding the complexities caused by the ORLs and its complications on patients, staff, and organizations. However, due to the restrictions of this assignment, the author will be focusing especially on the challenge of OR management and coordination. These issues will be explored in relation to the situation at the author’s hospital and a plan will be evaluated to make suggestions to sort this issue to improve future practice.
The situation at my workplace
In author’s hospital, most of the same-day cancellations of elective cases are caused by ORLs and consider as a complex issue and a daily debate in our department, as this lead to lots of problems, which negatively affect patients, staff, and the hospital. When the cancellation of surgeries occurs, the hospital does extra work rearranging the OR list and might need to reinvestigate the patient blood samples and x-rays. In addition, this will prolong the patients stay in the hospital leading to increase the treatment and medication costs. Thus, the ORLs will increase the patients and hospital costs (Boudreau and Gibson 2011). On the other hand, the OR staff will be requested to do extra times and be working under pressure to complete the scheduled operations in addition to the overbooked or canceled operations from previous days resulted in staff fatigue and staff dissatisfaction (Faiz et al. 2007). The latter thus negatively affect the working environment and the quality of service provided by the medical practitioners (AAGBI 2003).

In a recent effort to effectively resolve the ORLs at the author’s medical facility, the manager of OR tried to follow the international operations guidelines by restricting the time of operating lists to 8 hours (Pandit and Carey 2006). Nevertheless, this approach did not resolve the ORLs in the OR. As this is, a university hospital, which has quite some highly ranked professors with profound connections both internally and externally at the ministry levels, who used to manipulate the list and add new cases. Normally, the skilled professors would boldly carry out their oriented interests without taking in mind the complications of ORLs. For this reason, the intervention of the OR administration has failed, and the ORLs remains as a daily issue. Nevertheless, by looking at the management approaches at the author hospital, we can find a more influential remedy for ORLs.
Management
The ideal management ought to facilitate matters and promote competence to make the institution create better results (Daft 2012). Therefore, the medical facility’s administration and OR manager should use the most appropriate management strategies to be able to manage the scheduled of operating theaters lists (Higgins et al. 2013). Moreover, operational scheduling of OR, with an intention of subsiding costs and upholding a good quality of care delivered, has become priorities of the healthcare organizations (Jebal et al. 2006). Thus, an integrated management approach is needed by expending numerous management theories and models (Lee et al..1990). Hence, the following paragraphs will reflect on the most popular management theories (systems theory, contingency theory, and chaos theory) and their submission to the operating theater condition (Daft 2012).
Systems management approach
The system theory management looks to an organization as a large system consists of interconnected sub-systems (Rice 2013). Therefore, the management should analyze and facility the organization as a whole when they make decisions. On the other hand, decision-making should be oriented to the successive effects that a decision on one sub-system would have on other subsystems (Yoder 2014). Hence, the OR manager when making the schedule of operating theater should perceive it as a system consist of subsystems. The sub-systems include other sections that work in conjunction with the OR, other staff, patients, distributes instruments, equipment required and the entire hospital in general. Consequently, the decision and solution should be considered all aspect that the concerns of the stakeholders and other departments (Yoder 2014). As specified in the above situation analysis, the OR manager did not consider the situation of the patients, availability of special equipment, the variability in the staff skills and in some cases the surgeon need results from the laboratory which might take time (Faiz et al. 2007).
Contingency management theory
The contingency theory management stipulates that there is no perfect management remedy for each controlling issue faced by organizations (Van de Ven et al. 2013). Therefore, the organizations need to customize management approaches based on the status that the organization is facing currently (Lee et al..1990). By linking this theory to the situation of operating theater, it can be acknowledged that there is no ideal solution fit to all situation can be appropriate to ORLs, which consider challenges for the effective operation. The nature of cases that referred to the OR range between elective procedures, emergency cases, and major cases. Moreover, the different needs and prospects of workforce and patients, the availability of special tools are numerous factors that make it difficult for OR manager to establish a solution fit for all management strategy. Hence the OR manager required a contingent approach (Boudreau and Gibson 2011).
Chaos management theory
Chaos management theory points out that it is not possible to forecast systems, and the events indeed are rarely controlled. For this reason, it is difficult to plan a future for the organizations due to the wake of the profound dynamics, which influence organization (Arndt and Bigelow 2000). By looking to the fluctuating intricacy of the cases handled at the OR, it is of interest that the human resource understands the dynamics tangled and the inability of anyone to forecast the future (Yoder 2014). In this case, the surgeons have to line-up and respect the change of the 8 hours, which has been proved in previous studies and recommended by international associations (Pandit and Carey 2006).
Through the scrutiny of the three management approaches, can be recognized that there is a demand to understand the OR from the perspective of systems theory, support the utility of a contingency methodology, and escalate the dynamics included from the management perspective of chaos theory.
Suggestion plan
The solution of this issue should involve all the above management theory system. Pandit and Carey (2006) stated that the solution should take into account all the elements; the variability in the staff skills, cases that the surgeon has to wait for results from the laboratory, the patient’s status, availability of specific instruments. Moreover, Guinet and Chaabane (2003) propose that the OR manager should be considerate, especially when planning to perform the scheduled operation on a certain individual who in this case ought to have been cleared from the laboratory. Besides, it is recommended that the surgeon or the person in charge of the surgical operation ensure that all the necessary equipments are available and accessible prior to starting the procedure. The patient hospitalization date, as well as the surgery due time, should be profoundly considered to facilitate and promote a better patient satisfaction level. It is therefore suggested that the OR manager does the following.

Staff Meeting
According to Yoder (2014), the democratic leadership style can enhance the productivity. Thus, Braaf et al. (2013) stated that the OR manager should arrange a staff meeting to think of possible ways in which they can help to discourse the pertinent issues of ORLs in the medical organization. The ordinary time required for each surgery should be discussed and the time allowances that should be given for every case due to the occurrences of unexpected complication intraoperative. Moreover, the meeting not only for directors and managers but should include theatre staff to ensuring involvement of all stakeholders to assure contribution and pledge (Kotter 1998). However, patient safety must be the cornerstone for all decisions and changes recommended for any meeting of OR (Al Saffar 2011).
On the other hand, the medical practitioners including the surgeons, anesthetists, and the operation manager should adequately embrace the attribute of effective communication. The latter is regarded as a fundamental component in enhancing and pushing forward for a better and an outstanding healthcare setting as well as an elaborate patient satisfaction (Mutwali et al. 2016). In an operation theatre, for instance, tools and equipment’s will typically perform as they are supposed to, but there can be problems, which in this case might stem from the factors in between (Kosic, 2017). One of the best ways to address the complications that arise after the surgical operation has been carried is to profoundly initiate a better communication platform between the medics and the patients as well. By so doing, the medics can effectively and with utmost precision carry out the surgical procedure with minimal or no pitfalls in the spaces between them.
Patient safety has in the recent time been a primary component in promoting quality healthcare. In order to achieve a better patient safety and due to the complexity of the surgical procedures, the operation room ought to be managed and coordinated in a manner that secures the desired outcomes (Casinello, 2012). Teamwork capabilities may also incorporate non-technical skills that may aid the human personnel as well as the scientific training in acquiring the desired outcome with minimal or no shortcoming (Casinello, 2015). Clearly, established communication, coordination, and management is the crucial and utmost factors, which significantly aid in minimizing the surgical complexities in the various medical institutions (ORM, 2017).
Surgery type
Normally, patients scheduled for elective operations are highly affected by the cancellation of the surgical procedure, which in this is speculated to have been caused by lack of proper and adequate communication, coordination, and management channels (Kaddoum et al., 2016). On the other hand, the cancellation is accelerated by the state of the surgical procedure, which in this case is not urgently scheduled. The assumption adopted is that the cancellation of the procedure does not significantly affect the patient as compared to the cancellation of the in- elective procedure (Manolitzas, 2016, p 94).
Nevertheless, the latter is to a large degree not true because the cancellation of the surgical procedure highly inconveniences the patient and the people involved. Besides, the day of surgery cancellation initiates financial and logistics hardships and burden. This is because, upon cancellation of the procedure, the patient is prone to pre-operative preparations, prolonged stay in the medical facility, and the opportunity cost of lost time and income among many other factors. It is therefore wise that the medical facility management seeks and incorporate better ways of handling and carrying out their duties especially in the operation rooms. The latter can, however, be attained through the endorsement of proper communication between the medics and the patient, promotion of a sound coordination system between the medical practitioners, and eventually ensuring that the various facilities and department in the medical institution are sheltered and operate under a conducive and a favorable management body. By so doing, competency and patient satisfaction are guaranteed due to the reduced number of elective surgical operation.
Additional time
According to Macario (2010), it is a bit difficult to precisely predict the duration through which a surgical procedure requires in order to be comprehensively attended to. Notably, in some case, for instance, the surgeon and the operation room personnel might speculate on the average time required to complete the procedure, but they cannot exactly tell the minute the procedure will be completed.
In this regard, the operation room manager should take time and examine the patient’s condition or rather the surgical case in order to have an estimate of just how long an operation will last. Typically, the latter can only be possible by endorsing an established communication, management, and most importantly the coordination aspect of the operation room personnel.
By effectively incorporating the operation room personnel in examining the patient scheduled for surgery significantly aids in assessing his or her condition, which also helps in estimating the time required to complete the operation under normal conditions. On the other hand, by promoting the three primary aspects, coordination, management, and communication, the operation room personnel should be in a position to successfully complete the procedure regardless of any unexpected finding that may force the surgical procedure to consume some more time.
Use of statistical technique to facilitate efficient operating list scheduling
Normally, the operation room or rather theatres are primarily resourced with the skilled personnel including nurses and anesthetic only during the scheduled operation sessions (Leather, 2014). The operation room manager should, therefore, ensure that the operation room is equipped with the right facilities required to comprehensively and successfully complete the surgical procedure (Leather, 2014). This, nevertheless, can only be attained by setting up and embracing a better statistical analysis, which in this case should be built on a profound communication, coordination, and management platform (Dexter, Marsh, and Epstein, 2001).
Notably, adoption of a better statistical tool in the operation room management promotes efficiency through optimal theatre usage, which on the other hand maximizes the scheduled operation room time. As such, under-utilized time is minimized as well as the operating list that normally runs over the designated finish time. The Pearson correlation coefficient, for instance, should be adopted to evaluate the connection between the increasing operation procedures for all based on an operating list and session duration. Besides, it should aid in the provision of the operation list size and how long a single session duration. For all case and test that falls under p< 0.5 are regarded statistically relevant. It is therefore crucial that the operation manager maximizes the statistical tools in weighing and evaluating their progressive work entity.
Audit
The operation rooms sums to all huge investment of the health care facilities resources, which proportionally translates to quite a significant amount in the hospitals budget (Stavrou et al., 2014). This, therefore, imply that there is need to provide quality, competent, and efficient surgical and anesthetic procedures in the operation rooms. Nevertheless, cases of surgical cancellation on the scheduled day are increasingly on the rise due to suboptimal maximization and utilization of the operation room time and resources. In addition, inappropriate resource and personnel coordination, communication, and most importantly poor management also adequately push the frequent surgical cancellation forward.
In this regard, the operation room should thus initiate a better auditing platform through which a thorough assessment of the operation room resources as well as the incorporated personnel can be evaluated (Stavrou et al., 2014). On the other hand, adoption of a concrete auditing structure highly aids in time utilization, which in this case is oriented to a view of assessing the efficacy of the OR practices as well as identifying the areas that require more improvement (Stavrou et al., 2014). Typically, a progressive audit should frequently be carried out in the operation room in order to push forward for a better and a competent operation dynamic (Perkins et al., 2014). The latter should in return facilitate the initiation of proficient communication, coordination, and management human resource as defined in the contingency and chaos theory.
Change management theory to use
Change management theory is a crucial aspect of the organizational management for it ensures that all the departments in the vast organization are integrated as a way of attaining efficiency and customer satisfaction (Mulder, 2014). Notably, incorporation of the change management theory in the operation room would profoundly serve to boost coordination, communication, and the management aspect of the OR. Moreover, the operation room is also advised to integrate Kotter’s 8-stage model to effectively manage the suggested change in the medical facility.
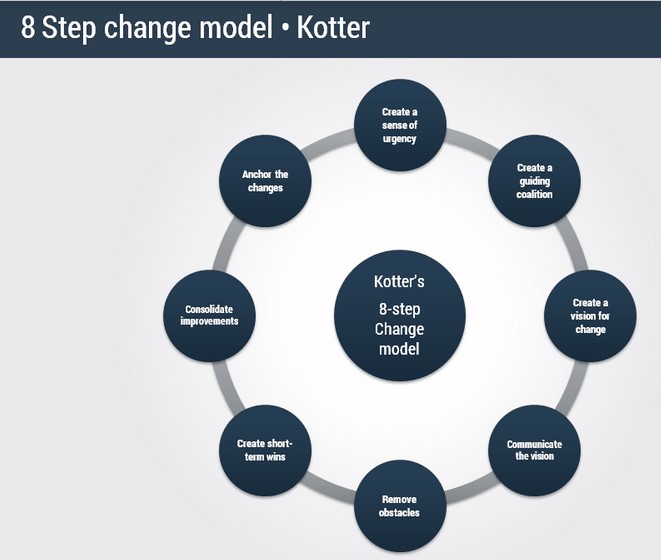
Figure 1 (Mulder, 2014).
Creating a sense of urgency
This is the first of the Kotter’s 8 steps. The operation room personnel should highly endorse the need of the patient in an urgent manner, which can be deployed through a better
and a convincing dialogue (Mulder, 2014). On the other hand, the ORM should try at all cost sensitize this issue in order to minimize or even avoid the potential threats that may arise in case the procedure is delayed.
Creating a guiding coalition
Coordination of the operation room personnel is a crucial aspect especially when positive changes are required. In this level, the operation room manager should boldly encourage the operation room skilled and non-skilled personnel to cooperate by availing all the required resources needed for carrying out the surgical procedure (Mulder, 2014). The OPM should also seek support from an influential organization in order to efficient increase the chances of successful change.
Communicate the vision
The operation room manager should thereafter incorporate the rightful stakeholders in establishing a concrete remedy regarding development and implementation (Mulder, 2014). By so doing, the operation room and the health facility at large ensure that there is a shared vision, which in return propagates positive chances of successful changes.
Communicating the strategy
Typically, the operation room manager in conjunction with the operation room personnel should ensure that all the initiated strategy in homogeneously shared among all the stakeholder as a way of evenly involving them in the course if change.
Broad-based action
This level calls for the involvement of all the stakeholders because it is an essential level where the developed and the implemented strategies and changes start to assume course (Mulder, 2014). It is therefore crucial that the operation room manager keenly observes and upholds this level.
Short term wins
Upon developing and implementing the various strategies, the operation manager shows frequently assess the progress in order to realize the potential loopholes as well as the pleasant change in the initiated strategy (Mulder, 2014). By so doing, the incorporated personnel and ion this case the operation room personnel will be in a position to know and credit the good work they have promoted in the designated timeframe. This sage is also termed as a motivational phase.
Consolidate gain
After the short terms have been credited, the operational manager should then adopt that as a platform and a base for future developments propagation (Mulder, 2014).
Anchor the new culture
Eventually, all progressive changes notable at each stage should be acknowledged and confined to the operation room culture (Mulder, 2014). The latter ensure that the notable change is positively sustained in the operation room entities.
Conclusion
In conclusion, operation management is a crucial and a sensitive aspect especially because human life is at stake. By incorporating and adhering to the various theories, the operation room manager should thus be in a position to effectively coordinate and manage the involved personnel in accomplishing the scheduled procedures. Typically, this would positively attribute to a reduction in the number of surgical operations that are rescheduled during their due date. Proper management would also minimize the run over the surgical procedures that have in the recent have exposed and even cost quite a significant number of individuals globally.
We can do it today.
- Al-Saffar, A., 2011. Enhancing Operating Theatre Efficiency of Private Hospital in Kuwait; Business Management Approach.
- Cassinello Plaza, F. (2017). The importance of teamwork in the operating rooms. [online] The Colombian Journal of Anesthesiology..
- Daft, R., 2012. Organization theory and design. Nelson Education.
- Dexter, F., Marsh, H. and Epstein, R. (2017). A statistical analysis of weekday operating room anesthesia group staffing costs at nine independently managed surgical suites. – Semantic Scholar. [online] Semanticscholar.org.
- Dimitriadis, P.A., Iyer, S. and Evgeniou, E., 2013. The challenge of cancellations on the day of surgery. International Journal of Surgery, 11(10), pp.1126-1130.
- Ezike, H.A., Ajuzieogu, V.O. and Amucheazi, A.O., 2011. Reasons for elective surgery cancellation in a referral hospital. Annals of medical and health sciences research, 1(2), pp.197-202.
- González‐Arévalo, A., Gómez‐Arnau, J.I., DelaCruz, F.J., Marzal, J.M., Ramírez, S., Corral, E.M. and García‐del‐Valle, S., 2009. Causes for cancellation of elective surgical procedures in a Spanish general hospital. Anaesthesia, 64(5), pp.487-493.
- Guinet, A. and Chaabane, S., 2003. Operating theatre planning. International Journal of Production Economics, 85(1), pp.69-81.
- Hovlid, E., Bukve, O., Haug, K., Aslaksen, A. and von Plessen, C. (2012). A new pathway for elective surgery to reduce cancellation rates. BMC Health Services Research, 12(1).
- Hovlid, E., Bukve, O., Haug, K., Aslaksen, A.B. and von Plessen, C., 2012. A new pathway for elective surgery to reduce cancellation rates. BMC health services research, 12(1), p.154.
- Ivarsson, B., Larsson, S. and Sjöberg, T., 2004. Postponed or cancelled heart operations from the patient’s perspective. Journal of nursing management, 12(1), pp.28-36.
- Jebali, A., Alouane, A.B.H. and Ladet, P., 2006. Operating rooms scheduling. International Journal of Production Economics, 99(1), pp.52-62.
- Jonnalagadda, R., Walrond, E.R., Hariharan, S., Walrond, M. and Prasad, C., 2005. Evaluation of the reasons for cancellations and delays of surgical procedures in a developing country. International journal of clinical practice, 59(6), pp.716-720.
- Kaddoum, R., Fadlallah, R., Hitti, E., EL-Jardali, F. and El Eid, G. (2016). Causes of cancellations on the day of surgery at a Tertiary Teaching Hospital. BMC Health Services Research, 16(1).
- Košič, K. (2017). Why Good Communication in the Operating Room is Important – ADORA. [online] ADORA.
- Kotter, J.P., 1998. Winning at change. Leader to leader, 1998(10), pp.27-33.
- Kumar, R. and Gandhi, R., 2012. Reasons for cancellation of operation on the day of intended surgery in a multidisciplinary 500 bedded hospital. Journal of Anaesthesiology Clinical Pharmacology, 28(1), p.66.
- Leather, A. (2014). Optimising operating list scheduling in the day surgery department: can statistical modelling help?.
- Macario, A. (2010). Is It Possible to Predict How Long a Surgery Will Last?. [online] Medscape.
- Manolitzas, P. (2016). Effective methods for modern healthcare service quality and evaluation. 1st ed. Hershey: IGI Global.
- Mulder, P. (2014). Kotter’s 8 Step Change Model: learn to lead organisational change | ToolsHero. [online] ToolsHero.
- Mutwali, I.M., Abbass, A.M., Elkheir, I.S., Arbab, S.S., Bur, A. and Geregandi, T., 2016. Cancellation of elective surgical operations in a teaching hospital at Khartoum Bahri, Sudan. Sudan Medical Monitor, 11(2), p.45.
- ORM (2017). Operating Room Management Research > Efficient Operating Rooms or not… This is the question ?. [online] Operatingroommanagement.org.
- Pandit, J.J., Westbury, S. and Pandit, M., 2007. The concept of surgical operating list ‘efficiency’: a formula to describe the term. Anaesthesia, 62(9), pp.895-903.
- Perkins, J., Chiang, T., Ruiz, A. and Prager, J. (2014). Auditing of operating room times: A quality improvement project. International Journal of Pediatric Otorhinolaryngology, 78(5), pp.782-786.
- Price, P., Frey, K.B. and Junge, T.L., 2004. Surgical technology for the surgical technologist: A positive care approach. Taylor & Francis.
- Rai, M.R. and Pandit, J.J., 2003. Day of surgery cancellations after nurse‐led pre‐assessment in an elective surgical centre: the first 2 years. Anaesthesia, 58(7), pp.692-699.
- Schuster, M., Neumann, C., Neumann, K., Braun, J., Geldner, G., Martin, J., Spies, C., Bauer, M. and CASCAES Study Group, 2011. The effect of hospital size and surgical service on case cancellation in elective surgery: results from a prospective multicenter study. Anesthesia & Analgesia, 113(3), pp.578-585.
- Stavrou, G., Panidis, S., Tsouskas, J., Tsaousi, G. and Kotzampassi, K. (2014). An Audit of Operating Room Time Utilization in a Teaching Hospital: Is There a Place for Improvement?. ISRN Surgery, 2014,